(Successful laparoscopic assisted myomectomy of a gigantic 9.4 kg uterine parasitic myoma: a case report and review of literature)
This blog is a continuation of Part 1, where we discussed diagnosis and risks of a giant fibroid.
ABSTRACT
Uterine leiomyomas are the most common benign tumours of the female pelvis affecting around 25-30% women of reproductive age. A case of successful laparoscopic assisted myomectomy in a giant uterine parasitic myoma is presented. A 42-year nulliparous morbidly obese lady presented with an Ultrasound diagnosis of a large uterine mass, detected during routine health check-up. MRI revealed a giant uterine pedunculated myoma of size 35 × 28 × 18 cm arising from the fundus and a 6 × 7 cm posterior wall myoma. After counselling the patient regarding surgical and anaesthesia risk, need of hysterectomy and laparotomy, laparoscopic myomectomy was planned. Laparoscopic findings revealed an exceptionally large parasitic fundal myoma filling the whole abdominal cavity and another 7 × 6 cm subserous myoma. main technical challenge was to tackle the big feeding vessels from the omentum providing massive blood supply to the gigantic tumor. Laparoscopic myomectomy was completed successfully using harmonic ace for coagulating the giant feeding vessels from the omentum. As the size of myoma was too big to put in the morcellation bag, so specimen retrieval was done through small incision and manual morcellation. The weight of the specimen was 9.4 Kg. This case emphasizes that size does not pose a limit to removing these gigantic myomas laparoscopically when surgical expertise and good anaesthesia facility is available. This is the case of largest myoma managed laparoscopically.
INTRODUCTION
Uterine leiomyomas are the most common benign tumours of the female pelvis affecting around 25 - 30% women of reproductive age. More than 50% patients are asymptomatic1. 1 Management of symptomatic myoma depends on the patient’s age, size and location of the myoma and future fertility issues.
Myomectomy is the best option in women requiring further fertility and uterine conservation. The advantages of laparoscopic approach are well proven and include smaller incision, shorter hospital stay, less subjectively reported postoperative pain, faster recovery and better assessment of the abdominal organs2. Limitations to laparoscopic approach include surgical expertise and need of suturing. Power morcellation further adds to the advantages of minimally invasive surgery to remove large myomas. Laparoscopic approach to huge myomas remains controversial and technically challenging. We present a case of asymptomatic giant parasitic myoma that was removed successfully through laparoscopy.
CASE REPORT
A 42-year nulliparous woman presented with diagnosis of a large uterine mass diagnosed incidentally on USG during routine health check-up.
Patient was asymptomatic and had no symptoms pertaining to this large myoma. On examination, patient was morbidly obese with weight of 117 Kg and BMI 42.8 kg/m2. Abdominal examination revealed a large uterine mass equal to term size gravid uterus with restricted mobility. To confirm the diagnosis, MRI was done which revealed a giant 35 × 28 × 18 cm subserous fibroid uterus arising from uterine fundus and another 7 × 6 cm subserous myoma in the posterior uterine wall (Figure 1).


The large myoma was extending up to hepatic surface displacing small intestinal loops and pancreas superiorly, retroperitoneal structures posteriorly and urinary bladder anteriorly. Her past medical and gynecological history was unremarkable.
The case was challenging in terms of gigantic size of myoma and route of surgery in this morbidly obese patient. After discussing the options with the patient, complete pre-anesthetic investigations and check-up was done. Laparoscopic myomectomy was planned to keep adequate blood products ready. The need and risk of laparotomy and hysterectomy was explained. Since putting the primary trocar above the fibroid was not possible, it was decided to put the primary port supraumblically mid-way between upper and lower margin of fibroid so that uterine attachment and feeding vessels can be visualized properly. Intra-operative findings revealed an exceptionally large myoma arising from uterine fundus and filling the entire abdomen (Figure 2). Manipulation of myoma and visualization of its attachment to uterus was a big challenge (Figure 3).

Another big challenge was large multiple feeding vessels coming from omentum which were the main source of blood supply to this giant parasitic myoma. The uterine attachment (about 5 cm pedicle), bilateral adnexa and other pelvic organs were visualized. Dilute vasopressin (20 units in 200 ml normal saline) was injected into the myometrium at the uterine attachment of myoma. The myoma was separated from the uterus using harmonic scalpel (Ethicon Endo-Surgery Inc, Cincinnati, OH, USA) and traction by myoma screw along with counter traction on the uterus. Myoma base was sutured using 1-0 V-loc unidirectional barbed suture (Covidien, UK). The challenge we faced while operating was the large serpentine feeding vessels (5-10 mm in diameter) from the omentum (Figure 4). These feeders were coagulated with bipolar coagulation and cut with harmonic scalpel.

Next big challenge was to remove this giant myoma. Putting the myoma into bag was not possible due to huge size. Keeping in mind the risk of morcellation related complications, decision was taken for manual morcellation. Lower port incision was enlarged to about 3 cm length and manual morcellation was done. At the end laparoscopy was done to check any residual pieces of myoma.
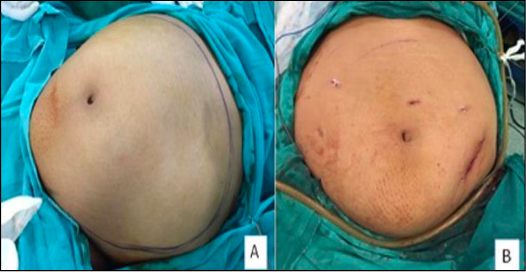

The procedure was completed in 4 hours with a blood loss of 700 ml. The weight of the specimen was 9.4 kg. Despite the difficulties faced there was no major intraoperative complications. Postoperative period was uneventful, and patient did not receive any blood transfusion. The patient was discharged after 48 hours. The final histopathological report was compatible with the diagnosis of a uterine leiomyoma. Pre-op and post op pictures of abdomen are shown in Figure 5. Figure 6 shows the morcellated pieces of myoma weighing 9.4 kg. The case has been approved by our hospital Institutional Review Board (IRB).
DISCUSSION
A myoma weighing 9.4 kg, filling the entire abdomen and successfully removed laparoscopically has not been reported in literature so far. Major hurdles and challenges in removing a gigantic myoma of this size are difficulties in finding the uterine attachment, finding cleavage plane, narrow operating space, specimen retrieval, repairing the myometrial defect, increased operative time, vascular injury to adjacent structures and conversion to laparotomy. Surgical options and approaches are not standardized, and the appropriate management of these very large myomas is complex and requires exceptional surgical skill, laparoscopic suturing and anaesthesia back up3. Laparoscopic myomectomy remains the gold standard of treatment for women harboring myomas that are in their reproductive age, infertile and wish to conserve their uteri. The removal of giant uterine leiomyomas is very rare, and literature is sparse with few case reports, largest measuring 21 cm and weighing 3400 g4. Yoon et al demonstrated the feasibility and efficiency of laparoscopic approach to large myomas and in their prospective study of 51 patients the largest removed myoma was 15.2 cm5. Table 1 shows the large myomas documented in literature which have been removed successfully through laparoscopic route. Our’s is the largest myoma among all the cases documented in literature removed successfully so far by laparoscopy.
| Authors | No. of patients | Size of myoma | Procedure | Weight of myoma |
|---|---|---|---|---|
| Sinha et al⁴ | Case series | 21 cm | Laparoscopic myomectomy | 3400 gm |
| Yoon et al⁵ | 51 patients | 15.2 cm | Laparoscopic myomectomy | 795 gm |
| Kavallaris et al¹⁰ | Case report | 18 cm | Laparoscopic myomectomy | 1200 gm |
| Ovali S et al¹¹ | Case report | 25 cm | Laparoscopic myomectomy | 1250 gm |
| Aksoy H et al³ | Case report | 17 cm | Laparoscopic myomectomy | 2005 gm |
| Present case | Case report | 33 × 28 × 18 cm | Laparoscopic myomectomy | 9400 gm |
One of the major concerns is the relationship of myoma with obesity and diabetes, where the common factor in this association is insulin resistance, elevated IGF-I and androgen levels6. Due to the decreased hepatic production of sex hormone binding globulin (SHBG) results in an increased bioavailability of estrogens and androgens7. In a study by He et al an increased risk of myomas was found in premenopausal women of Asian origin with a high BMI8. BMI of the present case was 42.8 kg/m2.
Another major concern in removal of large uterine myomas laparoscopically, is specimen retrieval. Morcellation can lead to inadvertent dispersal of myoma fragments in the abdominal cavity leading to benign and malignant complications e.g. parasitic myoma, disseminated leiomyomatosis and even occult malignancy and leiomyosarcoma. As such there is no method for predicting whether the myoma being removed is malignant so the US Food and Drug Administration (FDA) issued a statement of warning in November 2014 against the use of laparoscopic power morcellators in women undergoing hysterectomy or myomectomy for fibroid uterus. In Bag morcellation techniques have been devised to combat the risk of disseminating occult sarcomatous leiomyoma fragments throughout the abdominal cavity9. In present case, the myoma was too big to put into a morcellation bag. Manual morcellation was done keeping in mind the risk of occult malignancy in a giant myoma.
CONCLUSION
The case emphasizes that size does not pose a limit to removing these gigantic myomas laparoscopically when surgical expertise, efficient energy sources and anesthesia is available. This is the largest myoma removed successfully through laparoscopy as documented in literature.
Funding: No funding sources
Conflict of interest: None declared
Ethical approval: Not required
REFERENCES
Learn more about us by visiting this About page.
You can contact us by clicking this link.